CASE
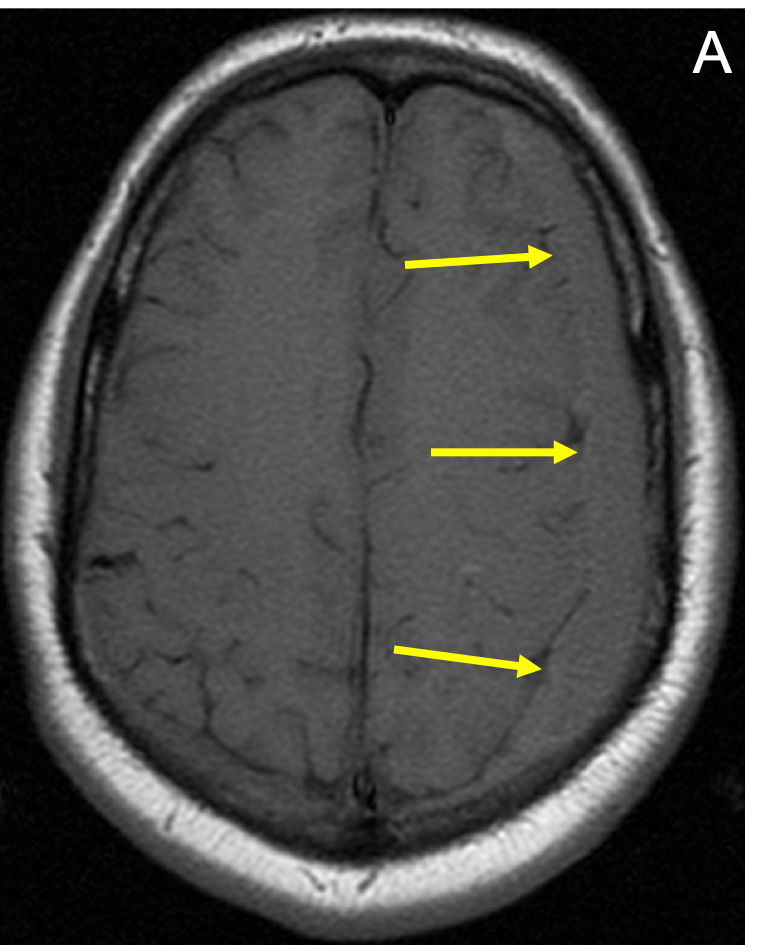
Brain – Subdural Hematoma (SDH)
CASE
22-year-old male with long-standing history of headache. Extraaxial fluid collection on left.
Long- and short-axis fat- and water-weighted images were obtained before and after contrast administration. 10cc of OptiMARK injected.

Learn from world renowned radiologists anytime, anywhere and practice on real, high-yield cases with Medality membership.

Try MRI Online Premium for free.
Unlimited
CME & SA-CME credits
Learn from world renowned radiologists anytime,
practice on real, high-yield cases with MRI Online Premium.