Diagnosis
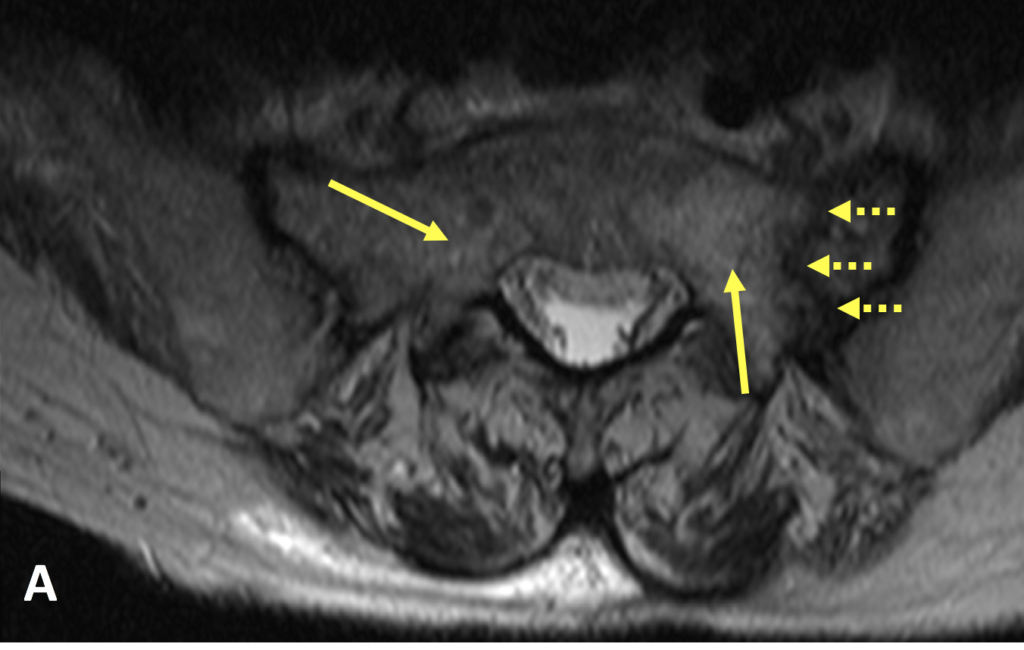
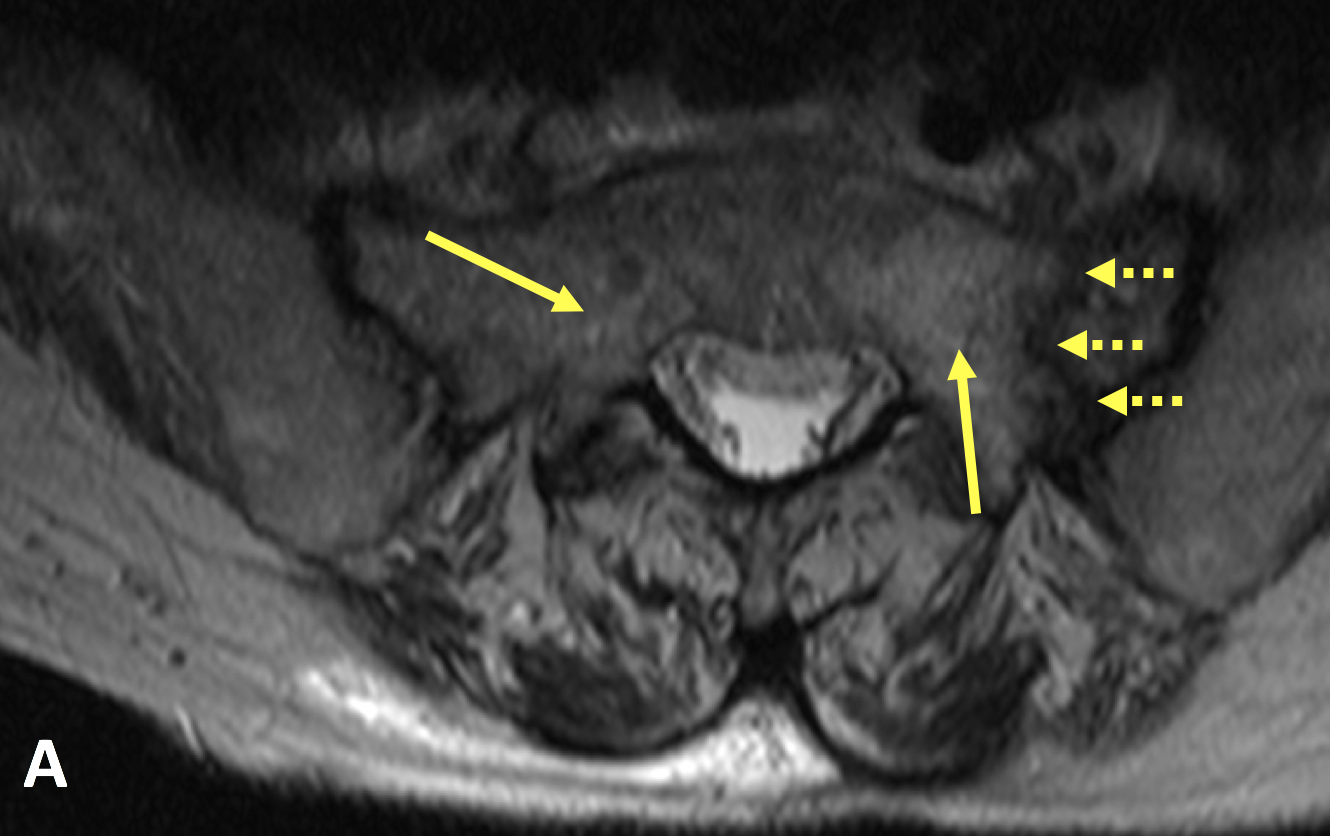
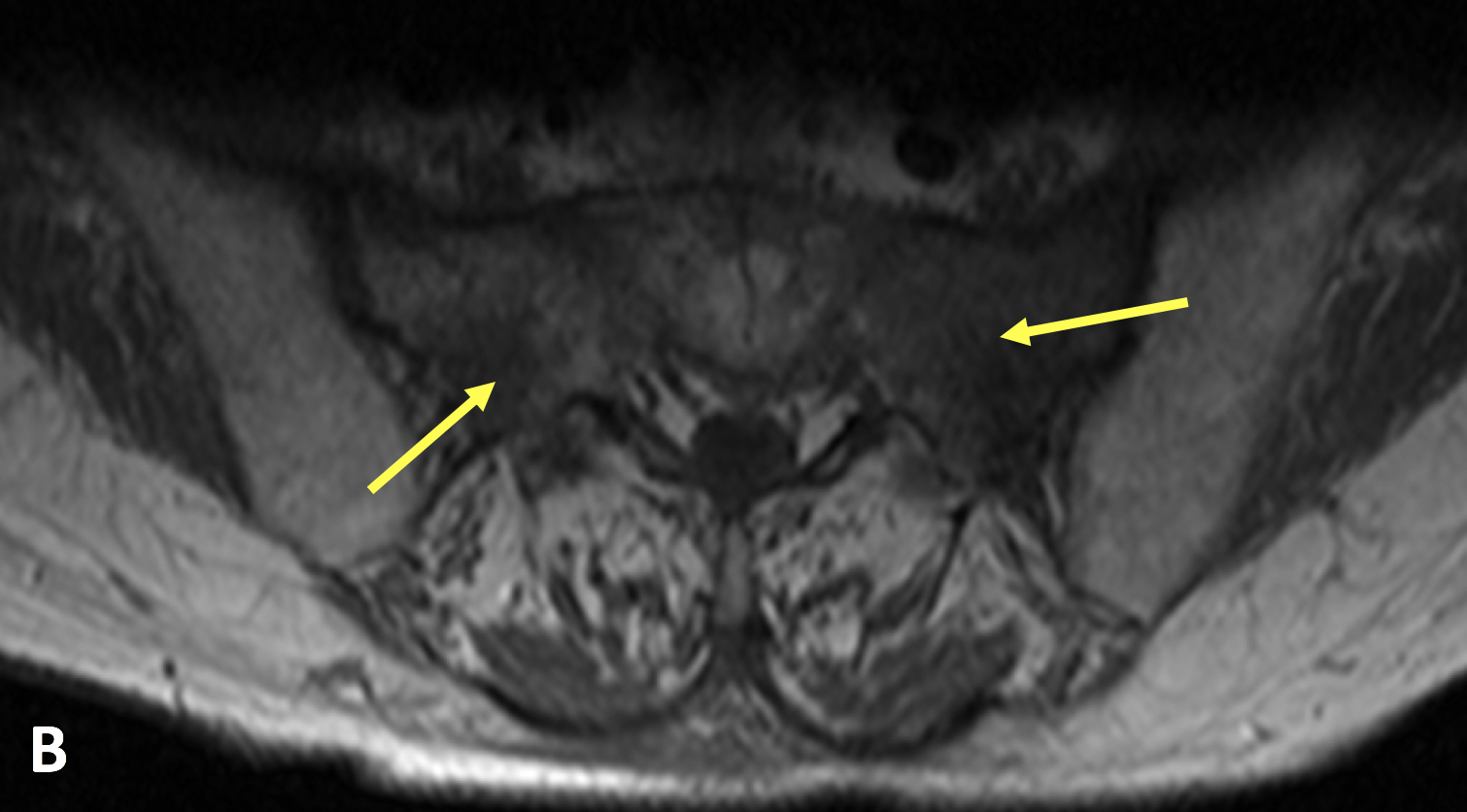
Sacral Insufficiency Fracture (SIF)
Diagnosis

Learn from world renowned radiologists anytime, anywhere and practice on real, high-yield cases with Medality membership.

Try MRI Online Premium for free.
Unlimited
CME & SA-CME credits
Learn from world renowned radiologists anytime,
practice on real, high-yield cases with MRI Online Premium.